Brain Aneurysm
Welcome to Dr Khurana’s Brain Aneurysm page.
Images shown here are with the permission of Dr Khurana’s patients, for educational purposes. There is a video example of an aneurysm clipping half way down this page.
Click any of the images below for a larger view.
Brain aneurysms are potentially lethal entities. They are effectively an outpouching or “berry” arising from a weakened part of a blood vessel’s wall. Most form without any specific reason, but their formation is known to be accelerated by smoking, high blood pressure, certain connective tissue disorders, and genetics running in some families.
Around 1-2% of people in the general population harbour one or more aneurysm(s), completely unaware. Fortunately, most brain aneurysms don’t cause a problem. Some, however, do, and the biggest problem associated with these is their rupture.
[For detailed information about brain aneurysms, please consider reading the reader-friendly book I co-wrote with Dr Robert Spetzler, entitled THE BRAIN ANEURYSM, sold and reviewed by purchasers at Amazon].
Below is a brief pictorial and videographic description for educational purposes.
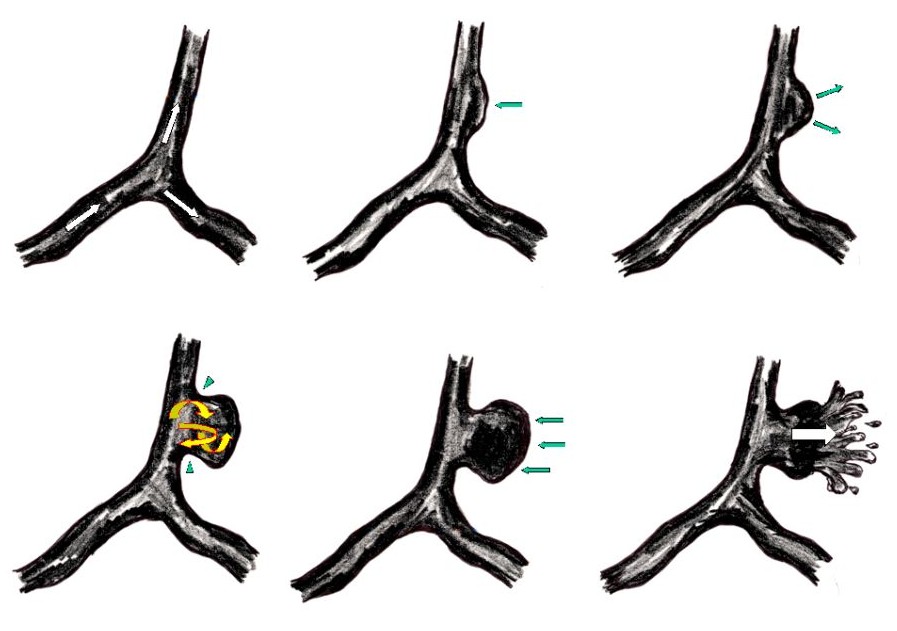
The figure below shows how an aneurysm arises from the wall of a blood vessel. It grows with time (green arrows), turbulent blood flow increases within its dome (yellow arrows), and eventually it further weakens and ruptures. Rupture (subarachnoid hemorrhage/SAH) presents as a sudden onset, super severe “thunderclap” headache; it can cause immediate loss of consciousness and in 10% sudden death from cardiac arrest. In around one-third of patients, the main rupture is preceded by one or more unusual “warning headaches”.
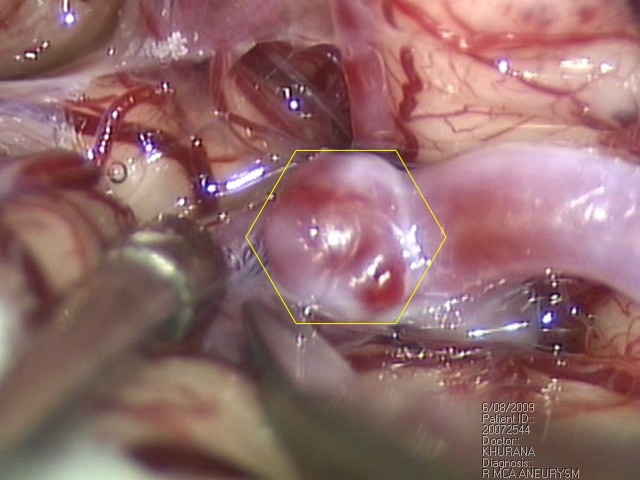
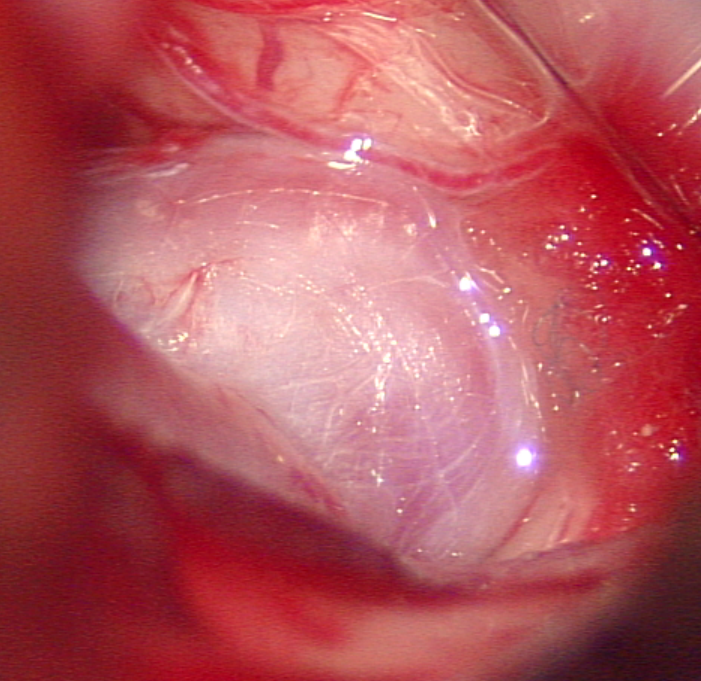
The fragile wall of an aneurysm is shown in this intraoperative photograph I took.
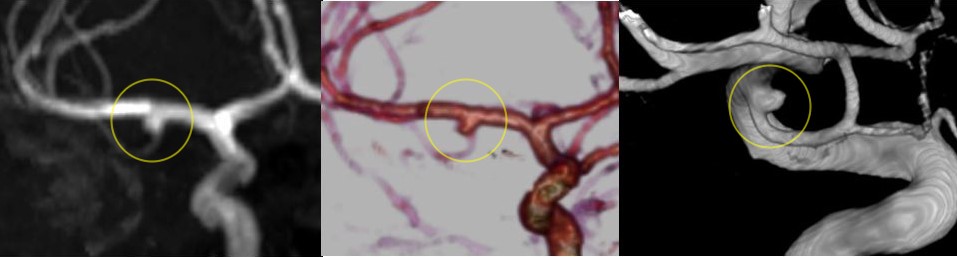
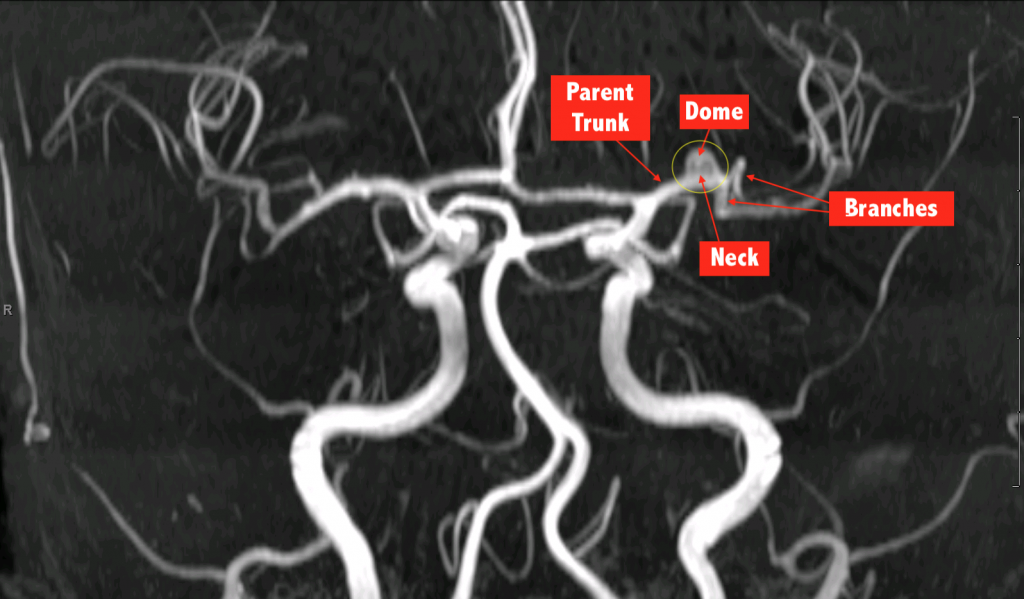
Aneurysms can be imaged by MR angiography (MRA), CT angiography (CTA) and the gold standard test known as catheter digital subtraction angiography (DSA). Each of these is shown respectively from left to right in the collage below.
Some aneurysms (green dotted circle in the MRA image below) have one or more ear-like projections off them called “daughter sacs” (red arrow tip below); these sites on aneurysms are thought to be even more prone to rupture. I recommend these be treated early.
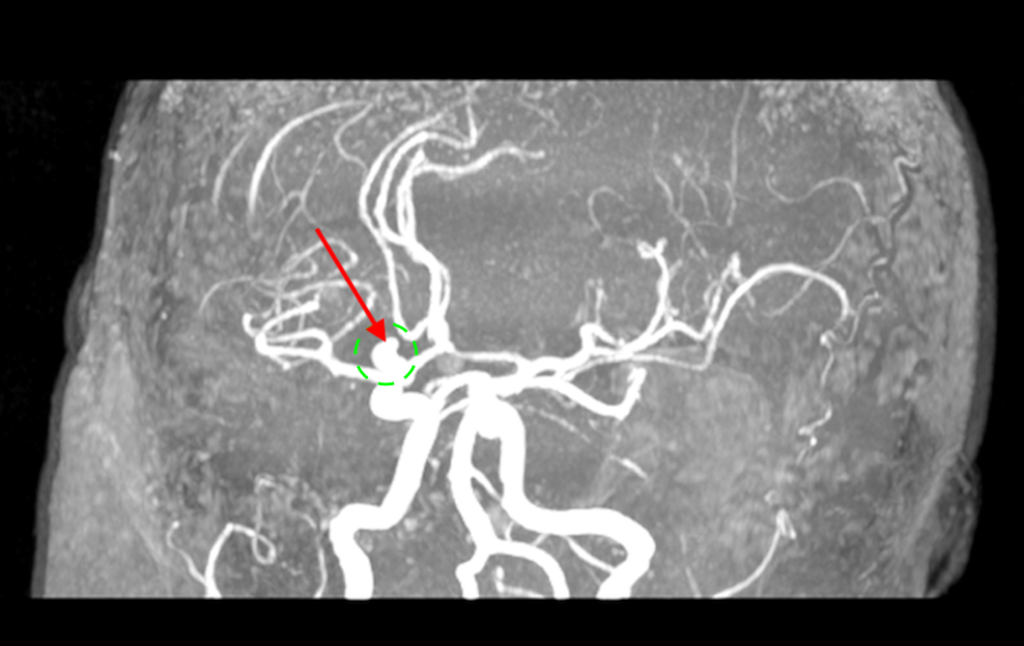
The “aspect ratio” has also been studied in aneurysms, and those with an aspect ratio (height of dome in mm divided by width of neck in mm) greater than 1.6 are also thought to be more prone to rupture.

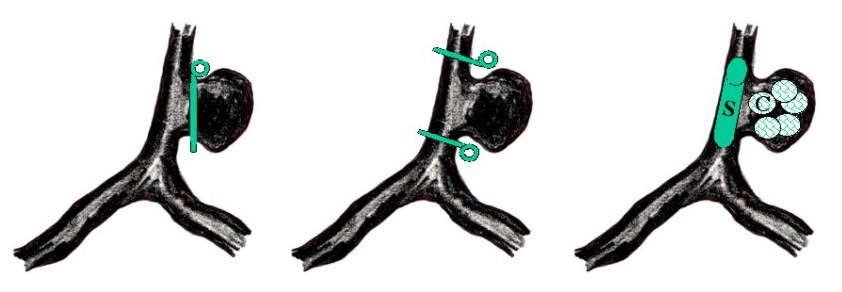
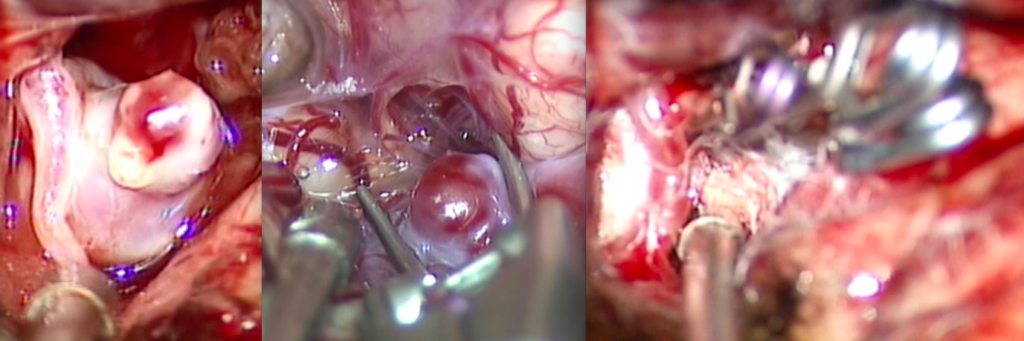
The treatment of aneurysms is mostly endovascular these days (“coil occlusion”, “coiling”, “stent-coiling”), by threading a catheter through the blood vessel(s) and into the aneurysm where the transported products are deployed. Some aneurysms (especially middle cerebral artery aneurysms) are still best treated by open microsurgery, via surgical clipping. The picture below illustrates the concept of treatment options: left – neck clipping; middle – parent artery trapping; right – stent (S) and coil (C) deployment.
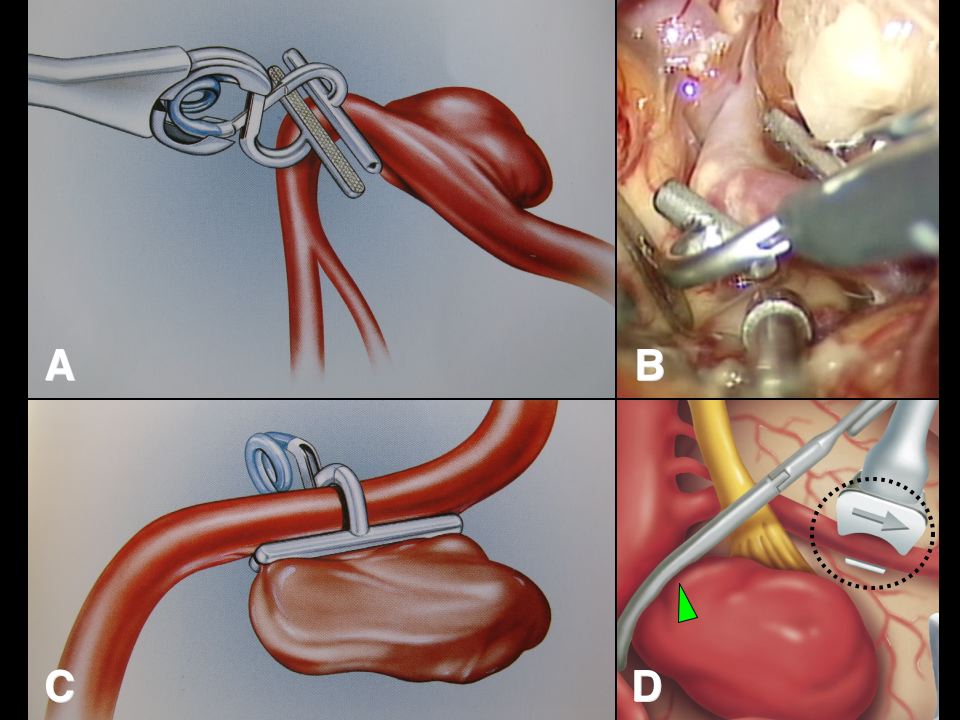
Here is a more elaborate picture, drawn professionally, of clip placement and intraoperative micro-ultrasonography in aneurysm surgery.
VIDEO EXAMPLE. Middle cerebral artery aneurysm:
This patient presented with an enlarging middle cerebral artery aneurysm. I sent her to an expert endovascular interventional radiologist; he thought this particular aneurysm was best treated microsurgically owing to its location close to main branches, and the shape and size of the aneurysm’s dome relative to its neck (“aspect ratio“).
The surgical trajectory to the aneurysm was planned using some amazing software and hardware (3D CTA DICOM data set, BrainLab Curve).
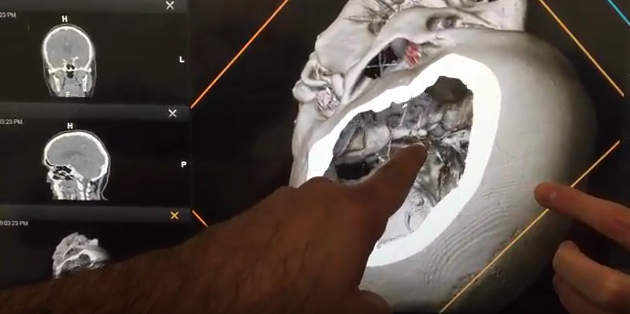
CLICK HERE for surgical planning video (YouTube Clip #1 of 5; t=41 secs).
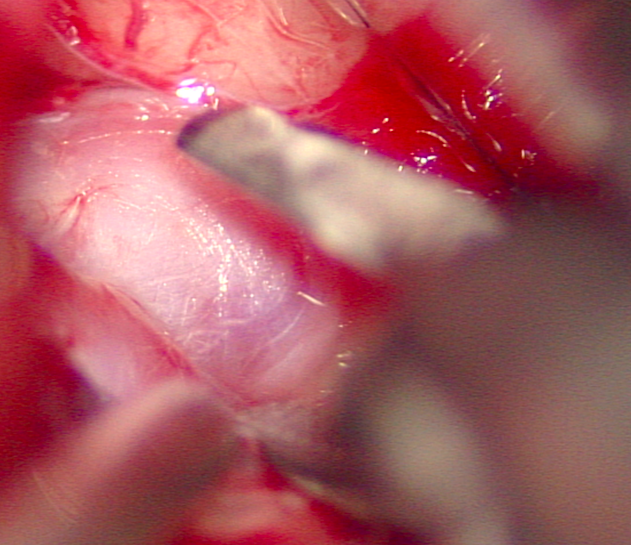
The aneurysm was microsurgically exposed.
CLICK HERE for surgical exposure video (YouTube Clip #2 of 5; t=54 secs).
Prior to clipping, I carried out fluorescence angiography (ICG-VA) to best appreciate the local blood vessel anatomy and blood flow prior to the aneurysm’s clipping.
CLICK HERE for the pre-clipping ICG-VA video (YouTube Clip #3 of 5; t=18 secs).
The aneurysm was then clipped using a B.Braun/Aesculap bayoneted straight titanium permanent microclip placed across the neck of the aneurysm without compromising the local blood vessels (parent artery and its branches).
CLICK HERE for the clipping video (YouTube Clip #4 of 5; t=47 secs).
At the end of the procedure and prior to surgical closure, I carried out post-clipping ICG-VA to confirm that the local blood vessels were AOK, and the aneurysm was obliterated.
CLICK HERE for the post-clipping ICG-VA video (YouTube Clip #5 of 5; t=15 secs).
The patient was uneventfully discharged from hospital a few days later. Mission accomplished!
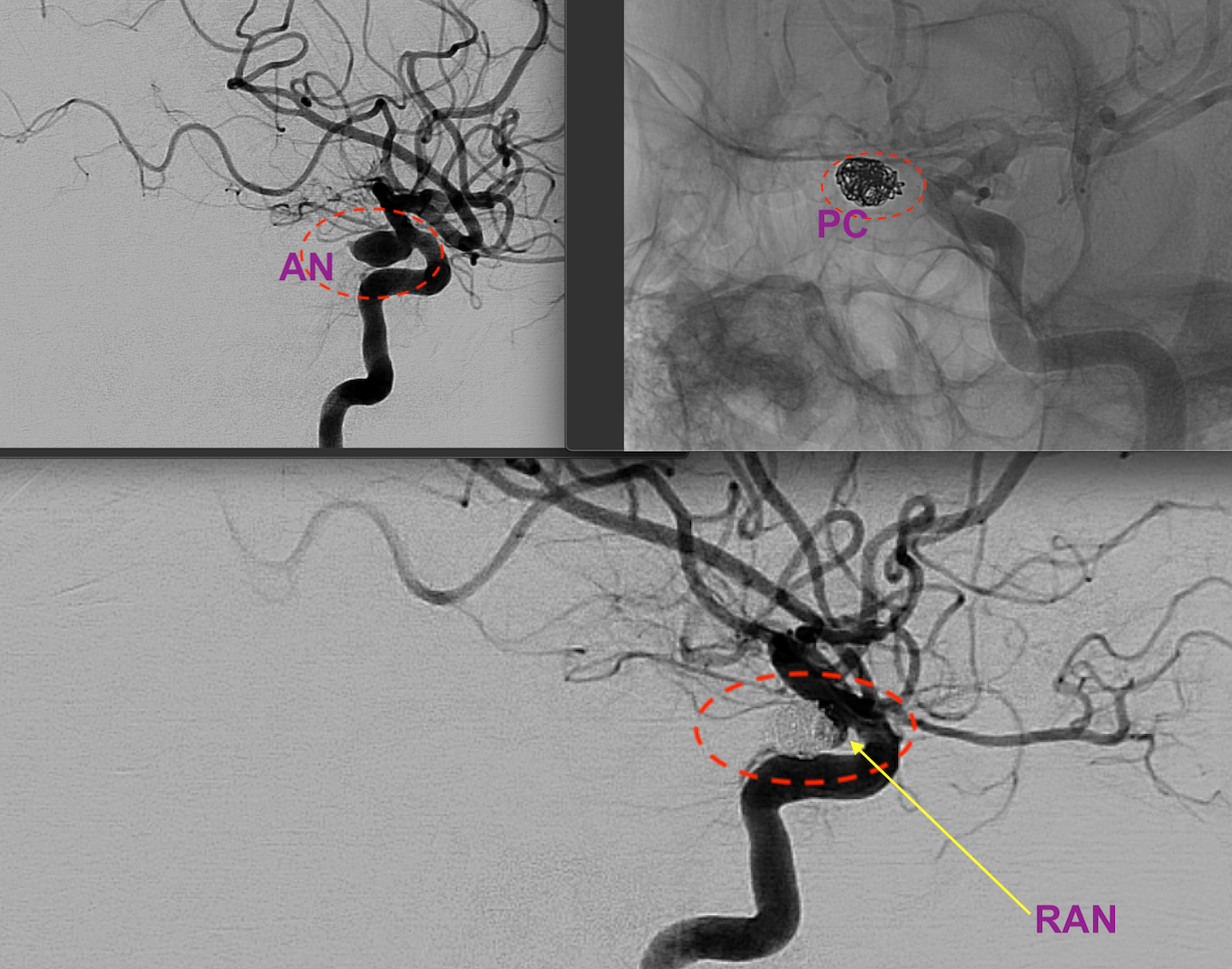
Aneurysm (AN) shown below was endovascularly packed with coils (PC) after its hemorrrhage (SAH), and the patient’s life was saved. However, some “recanalisation” of the neck region (RAN) occurred (i.e., the aneurysm started to fill again at the neck region after initially apparently successful coiling). As this posed a risk of growth and re-haemorrhage, it needed to be re-treated. The options discussed were: 1. Flow-diverting stent across the neck (the solid wall stent can shut down the neck region but can sometimes entrap small local arteries, if any are present); 2. Perforated stent-coiling (i.e., further coiling of the residual part of the aneurysm through a perforated stent’s tiny openings); 3. Attempted surgical clipping of the neck (the surgeon should expect residual coils in the neck).
If you have any questions about your situation, feel free to contact us for a consultation via the details on our Contact page